Regression of clubbing can occur after corrective surgery for cyanotic congenital heart disease as they become acyanotic after surgery.
Regression of clubbing after treatment of lung cancer is well
Most of the musculoskeletal disorders are more prevalent in females. e.g. Osteoarthritis of knee, Fibromyalgia, Rheumatoid arthritis, Polymyalgia rheumatica
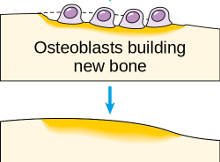
Bone remodelling is the process by which mature bone is removed via resorption and replaced with new bone. It is a process which continues throughout life.
Biomarker least useful in diagnosis of myocardial re-infarction: a) Troponin I b) CPKMB c) Myoglobin d) CPK Click here for the answer Prof. Dr. Johnson Francis, MD,
Biomarker least useful in diagnosis of myocardial re-infarction: Answer: a) Troponin I Diagnostic troponin elevations can be seen within six hours, but the values remain in diagnostic range
Increased E point – septal separation (EPSS) on M-mode echocardiogram of mitral valve is indicative of : a) Mitral stenosis b) Mitral regurgitation c) Left ventricular dysfunction d)
PG Blazer is aimed at helping undergraduate medical students in acquiring more knowledge and increasing their chance of getting admission to postgraduate courses by performing well in the post graduate medical entrance examinations. Students are requested verify the accuracy of information in standard text books. This site is not meant for any medical advice or treatment. Please contact your physician for medical advice and treatment.